At
Boulder Valley Surgical Associates (BVSA), our experienced general surgeons and trauma surgeons treat a wide variety
of hernia types, each affecting the abdomen, abdominal wall, diaphragm
or stomach. These repairs can be performed using traditional open approaches,
advanced laparoscopic techniques or minimally invasive robotic surgery with the
da Vinci system.
What is an abdominal wall hernia?
When a hernia occurs, an internal organ such as the intestine or fatty
tissue pushes through the abdominal wall via a weak spot in the musculature.
“At its most basic level, a hernia is a defect or a hole in the abdominal
wall, whether that’s from natural development versus incisional
hernias from previous surgeries,” says BVSA general surgeon
Kyle Marthaller, MD, FACS.
Someone with a hernia will have a visible lump, pain or burning sensations,
particularly when straining or standing. Hernias do not go away on their
own, so most are treated via surgical repair.
“Between the mesh types, suture types and types of (surgical) techniques,
I can probably combine 100s of different ways to fix a hernia,”
says BVSA general surgeon
Bulent Cetindag, MD, FACS. “It all depends on the patient’s goal.”
It is our honor to know our team can assist you or your family with some
of life’s significant challenges. To make a consultation appointment
with one of the BVSA surgeons, call
303-415-4599.
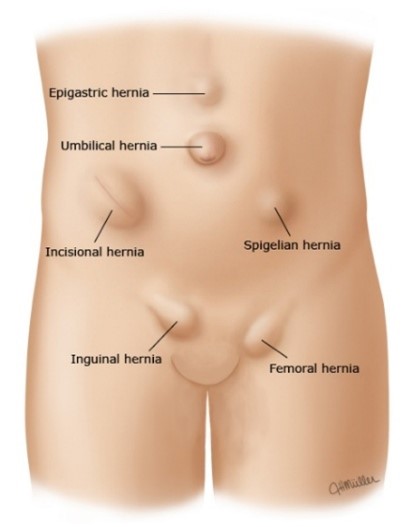
Inguinal (groin) and femoral hernias: An inguinal hernia is a bulging of the abdomen’s contents through
a weak area in the groin area. Inguinal hernias are much more common in
men, but also do occur in women. Femoral hernias occur much more frequently
in women and are located below the inguinal ligament, which is also part
of the groin area.
Umbilical (belly button) and epigastric hernias: These are types of ventral hernias, which are in the front of the abdominal wall.
Incisional hernias: These hernias occur at the site of a previous abdominal procedure. In developed
countries, such as the United States, abdominal surgeries are common and
create weak points in the abdominal wall. People who have had prior abdominal
operations have up to a 20% chance of developing a hernia in their previous incision.
Hiatal hernias: A
hiatal hernia happens when part of the stomach pushes up through the diaphragm (the
muscle that separates the chest from the abdomen) into the chest cavity.
Learn more about hiatal hernias
here.
Rare hernia types: Flank, lumbar (back of abdomen), obturatoror and spigelian.
Approximately 611,000 ventral and one million inguinal hernia repairs occur
annually in the United States, with more than 20 million performed worldwide,
making hernia repair one of the most common general surgical conditions globally.
How do you develop a hernia?
Common risks include heavy lifting, obesity, chronic coughing and previous
surgical scars.
Acquired risk factors: Smoking, obesity/body mass index (BMI) of 35 or higher, lung disease or
chronic cough, poor nutrition, pregnancy, chronic heavy lifting, enlarged
prostate/other urinary tract obstructions, chronic constipation, previous
abdominal surgery/presence of ostomy, and chronic use of corticosteroids.
Congenital risk factors: Male gender (especially for groin hernias), undescended testicles, and
family history of genetic disorders of connective tissue and collagen.
Symptoms of a hernia
Many patients do not have symptoms, and the hernia is discovered by a provider.
Visual lump
Sharp pain with activity (coughing or lifting)
Dull, aching pain at rest (especially after standing or walking) associated
with a lump.
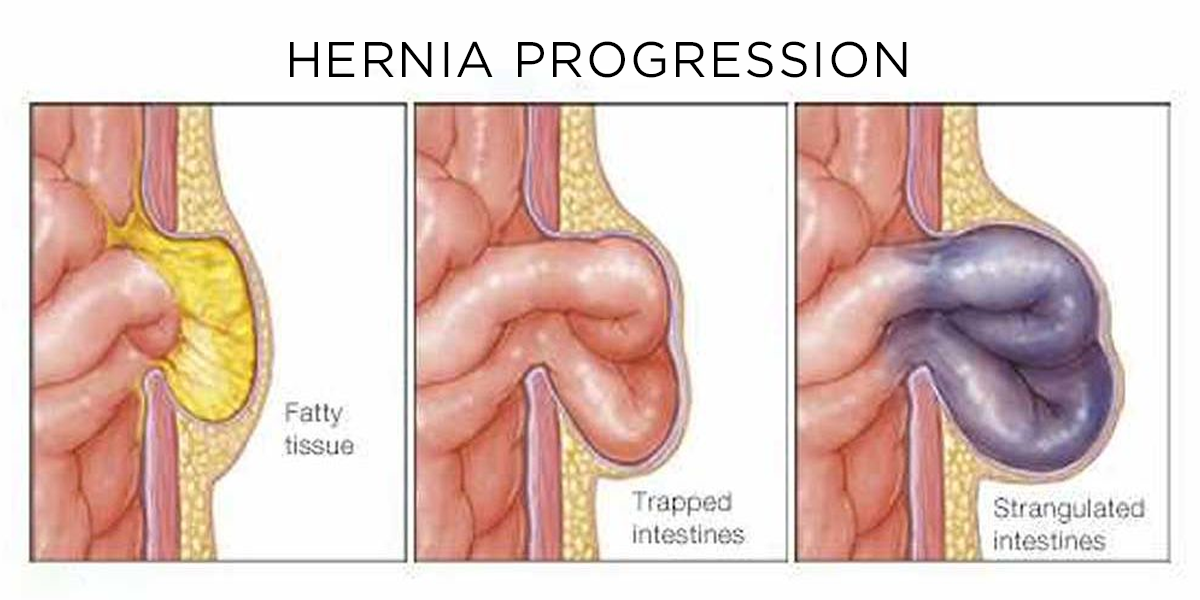
If a bulge from hernia is stuck and painful, this can be an emergency.
A visit to the emergency department (ED) is recommended to avoid damage
to the intestines. This is also known as an incarcerated hernia –
herniated tissue that becomes trapped and cannot easily be moved back
into place.
Urination problems if the bladder is inside the hernia. This is exceedingly rare.
Diagnosing a hernia
Physical exam by a qualified health care provider can be sufficient to
diagnose a hernia.
Potentially needed imaging studies:
Ultrasound – This can usually diagnose most hernias if the diagnosis cannot
be made via physical exam. There is no radiation when using ultrasounds.
CT Scan – May be needed for operative planning on complex hernias.
MRI – Occasionally used to diagnose a sports hernia when the symptoms
are groin or nerve pain.
Treatment options
Watchful waiting can be an option for a small hernia that is not causing symptoms.
Elective surgery can be performed to fix hernias that have higher risk
features or cause symptoms. The principal of all hernia repairs is the
same: The contents of the hernia are placed back in the abdominal cavity
and the hole in the musculature is closed or reinforced, often with mesh.
Emergency surgery is necessary for incarcerated or strangulated hernias
when bowel or other organs are trapped in the hernia and losing their
blood supply.
Surgical approaches, mesh materials/placement and anesthesia
These decisions are made between each individual patient and surgeon. Your
surgeon will offer recommendations based on age, gender, pregnancy, activity
levels, lifestyle goals and hernia size.
“The beauty of hernia repair is that it’s not a cookie-cutter
approach to each patient; there’s multiple different modalities
to approach the hernia, whether that’s minimally invasive or open,”
says Dr. Marthaller. “And then there’s multiple ways to fix
the hernia, whether through sutures or using a mesh repair.”
Approaches: Robotic, laparoscopic or open
Local anesthesia: For open inguinal hernia repair
Mesh material: Synthetic, bioabsorbable, biologic or hybrid
Our surgeons try not to use mesh for ventral hernias less than 2cm.
Mesh placement: Onlay, inlay, retromuscular, preperitoneal or intraperitoneal
Anesthesia:
General – Loss of consciousness; unable to feel pain.
Sedation - Monitored Anesthesia Care/MAC, or "twilight sedation," is a
tailored anesthesia service where an anesthesia provider administers sedatives
and analgesics to keep patients calm, comfortable and pain-free during
minor procedures.
Local - Numbs a small, specific area of the body. The patient remains fully awake
and alert. With hernia surgery, we work with our anesthesia colleagues
and use sedation or general anesthesia depending on the repair.
“The mesh that we use today has changed significantly; it is still
mostly nonabsorbable, but there are absorbable options as well,”
says. Dr. Marthaller. “The mesh has evolved from a (rigid) plastic
type of material to more of a cloth-like material that tends to work better
with people’s own anatomy.”
Inguinal hernia repair without general anesthesia
Although 80% of inguinal hernias in the U.S. are repaired using general
anesthesia, our general surgeons can perform inguinal hernia repairs using
an open surgery approach paired with light sedation. For older adults
who have other health problems, this can improve recovery. A 2022
study also found that using local rather than general anesthesia for inguinal
hernia surgery was associated with significantly fewer complications and
less time in the operating room and post-anesthesia care units, regardless
of patient age. However, this is only available for an open repair.
If you are interested in inguinal hernia repair without general anesthesia,
schedule a consultation with any BVSA surgeon by calling
303-415-4599.
What to expect after hernia surgery
While there are no activity restrictions prior to surgery, there are several
things’ patients need to be familiar with post-surgery.
Pain is typically mild to moderate and manageable.
Most post- operative pain can be managed with over-the-counter pain medication.
Your surgeon may recommend activity restrictions immediately after your
operation.
Patients often return to normal activities within a few weeks.
How you feel during your post-operative recovery will depend on the type
of hernia repair you and your surgeon choose and would be discussed at
your consultation.
Want to learn more about hernias? Watch our latest lecture.
Make a consultation appointment
It is our honor to know our team can assist you or your family with some
of life’s significant challenges. To make a consultation appointment
with one of the BVSA surgeons, call
303-415-4599.